




The information in this section will help you to understand the fundamentals of recognising, referring and supporting a patient with an interstitial lung disease in primary care.
This is not a substitute for completing an appropriate respiratory assessment module. For advice and support on choosing the right course for you, please see our training and development page.
Interstitial Lung Diseases
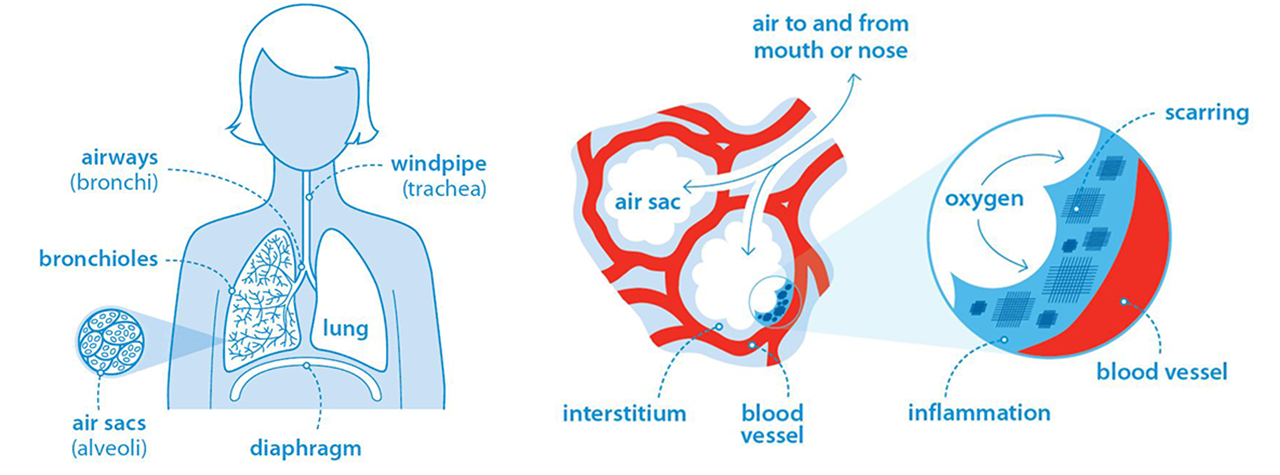
Interstitial Lung Diseases (ILDs) are a group of over 200 diseases that cause scarring (fibrosis) or inflammation in the lung parenchyma. Some interstitial lung diseases cause the interstitial lung tissue to become stiff and thickened, or scarred. This is known as pulmonary fibrosis.
The lung parenchyma refers to the part of the lungs involved in gas exchange. It primarily includes:
Alveoli: The tiny air sacs where oxygen is absorbed into the bloodstream and carbon dioxide is removed.
Bronchioles: The small airways that lead to the alveoli, responsible for carrying air to the alveoli spaces.
Interstitial Tissue: The supportive connective tissue surrounding the alveoli and small airways, which provides structure to the lungs and plays a role in gas exchange.
Fibrotic ILDs are restrictive lung diseases because scarring reduces lung volume and limits the lungs' ability to expand fully during inspiration.
They differ from obstructive lung diseases such as asthma and COPD, in which narrowed airways make it difficult to fully exhale air from the lungs.
It is possible to have both obstruction and restriction if a patient has an ILD in addition to a condition such as asthma or COPD.
Some ILDs are progressive, meaning that fibrosis develops and worsens over time, while others remain relatively stable. Progressive fibrosing ILDs are associated with a poorer prognosis and can lead to worsening symptoms, declining lung function and reduced quality of life.
Not all ILDs result in permanent fibrosis. Some are predominantly inflammatory and may respond well to treatment. Prompt diagnosis and management can help control inflammation, improve symptoms and, in some cases, reduce the risk of progression to irreversible lung damage.
This is why it is important that patients with suspected ILD are recognised in primary care and referred promptly for further investigation and specialist assessment.
Symptoms of ILD to look out for in patients
Signs and symptoms include:
- Gradual breathlessness which is worse on exertion
- A persistent cough every day lasting for more than 8 weeks, often but not always, dry
- Fatigue
- Unintentional weight loss
- Bilateral inspiratory 'velcro' crackles when listening to the chest
- Clubbing of the fingers.
Causes and risk factors for ILD
For many patients with an ILD, there is no clearly identifiable cause. This is known as an idiopathic ILD.
Patients who are more likely to have interstitial lung disease (ILD) tend to fall into several high-risk categories based on a combination of age, medical history, environmental exposure, and lifestyle factors. The following groups are at increased risk:
1. Older adults
Age is a significant risk factor for many forms of ILD, especially idiopathic pulmonary fibrosis which predominantly affects people aged over 50 years.
2. Patients with connective tissue diseases
People with autoimmune conditions, such as rheumatoid arthritis, systemic sclerosis and systemic lupus erythematosus, are at higher risk of developing connective tissue disease-associated ILD.
3. Smokers or ex-smokers
Smoking significantly increases the risk of developing certain types of ILD, including respiratory bronchiolitis-associated ILD and idiopathic pulmonary fibrosis.
4. Occupational and environmental exposures
Patients with long-term exposure to certain inhalants, such as asbestos, silica, coal dust, mold, and bird proteins, are at risk of developing forms of ILD like asbestosis, hypersensitivity pneumonitis, or pneumoconiosis.
5. Medication
Certain medications, including chemotherapy agents (such as bleomycin), antiarrhythmic drugs (such as amiodarone) and antibiotics (such as nitrofurantoin), are associated with interstitial lung disease.
6. Patients with family history of ILD
Individuals with a family history of ILD, particularly idiopathic pulmonary fibrosis, are at greater risk of developing the disease.
7. Gastroesophageal reflux disease (GORD)
Gastro-oesophageal reflux disease (GORD) is common in people with idiopathic pulmonary fibrosis (IPF). Stomach contents may sometimes enter the lungs (microaspiration), which may contribute to lung damage and disease progression.
Types of ILD
The most common ILDs include:
- Idiopathic pulmonary fibrosis
- Sarcoidosis
- Extrinsic allergic alveolitis (also known as hypersensitivity pneumonitis)
- Interstitial lung disease associated with connective tissue disease
- Pneumoconiosis
- Interstitial lung disease caused by certain drugs used to treat other conditions.
Patient outcomes for ILD
Outcomes in ILD vary depending on the underlying condition, disease severity, rate of progression and response to treatment. Inflammatory ILDs often have a more favourable outlook than fibrotic ILDs because inflammation may be partially reversible if identified and treated early.
Some people experience an improvement in symptoms and stabilisation of lung function, while others may go on to develop permanent lung scarring.
Progressive pulmonary fibrosis (PPF) is a life limiting condition for which there is currently no cure. Prognosis varies considerably depending on the underlying type of ILD, the severity and rate of disease progression, age, coexisting conditions and access to treatment. Some individuals may remain stable for many years, while others experience more rapid disease progression.
Idiopathic pulmonary fibrosis (IPF) is the most common form of progressive fibrotic ILD. Historically, median survival following diagnosis was estimated at around 3 to 5 years.
However, these estimates were based on data collected before the introduction of antifibrotic therapies, which can slow disease progression. Many people now live longer than historical survival estimates would suggest.
Living with pulmonary fibrosis

Watch John's story of living with IPF
Pulmonary fibrosis can have a profound impact on a person's physical health, emotional wellbeing and quality of life. As symptoms worsen, many people experience increasing breathlessness, fatigue and limitations in their daily activities.
In this video, John shares his experience of living with idiopathic pulmonary fibrosis (IPF), from diagnosis through to managing the impact of the disease on everyday life.